Thoracic Trauma Pneumothorax - Tension
Tension Pneumothorax
Tension pneumothorax is the progressive build-up of air within the pleural space, usually due to a lung laceration which allows air to escape into the pleural space but not to return. Positive pressure ventilation may exacerbate (worsen) this 'one-way-valve' effect.
Progressive build-up of pressure in the pleural space pushes the mediastinum to the opposite hemithorax, and obstructs venous return (Inferior and superior vena cava) to the heart. This leads to circulatory instability and may result in traumatic arrest. The classic signs of a tension pneumothorax are deviation of the trachea away from the side with the tension, a hyper-expanded chest, an increased percussion note and a hyper-expanded chest that moves little with respiration.
However these classic signs are usually absent and more commonly the patient is tachycardic and tachypneic, and may be hypoxic. These signs are followed by circulatory collapse with hypotension and subsequent traumatic arrest with pulseless electrical activity (PEA). Breath sounds may be very difficult to interpret and misleading in the high noise environment of the field. There may also be "referred' sounds from the uninjured side that further complicates diagnosis.
Tension pneumothorax may develop insidiously (slowly, without obvious symptoms at first, so that the person is not aware of it developing), especially in patients (COPD, trauma. Asthma) with positive pressure ventilation (BVM / CPAP). This may happen immediately or some hours down the line. An unexplained tachycardia, hypotension and rise in airway pressure are strongly suggestive of
a developing tension pneumothorax.
Left side tension pneumothorax. Note that heat is displaced to patients right side. Also trachea is shifted to right (away from side with pneumothorax).

EMS Treatment of a Tension Pneumothorax
Note: The information in this section are general guidelines and should be consider permission or instruction in actual patient care. Follow your local guidelines and medical control in all situations.
- BLS treatment
- O2, rapid transport to trauma center
- If open (sucking) chest wound consider sealing on three side with occlusive dressing or using commercial sealing device.
- If patient's condition deteriorates after sealing with occlusive dressing remove dressing and see if patient's condition improves.
- Avoid positive pressure ventilation if at all possible.
- ALS treatment
- All of the above
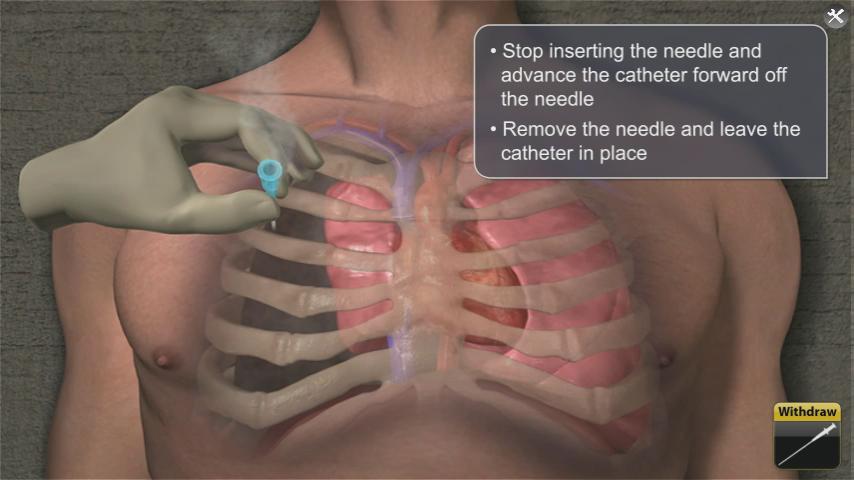
- Consider needle Thoracostomy over affected lung to relieve pressure
- 2nd intercostal space (Between 2nd and 3rd rib). Insert needle superior to 3rd rib to avoid neuro-vascular bundle under 2nd rid.
- Continue to monitor patient.
Open or sucking chest wound

Occlusive dressing

Asherman chest seal

Bolin Chest seal

SAM chest seal

Needle Thoracostomy (ALS Level)

Needle Thoracostomy land marking (2nd intercostal space)
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.